The Pathway from Screening to Diagnosis
After a positive screen, you will be contacted by a healthcare professional who specialises in caring for children with SMA. You are offered an appointment at a specialist centre with a paediatric neurologist. For families living in rural and remote parts of Australia and New Zealand this may be with your local healthcare professional via video chat.
We know it can be hard to act quickly, but it is important. If needed, you can bring a support person to help you.
At this appointment member/s of your healthcare team will:
- examine your baby,
- talk to you about SMA
- organise diagnostic tests. These include tests to also understand how SMA may impact your baby.
Treatment options can begin to be discussed at this appointment. Sometimes blood tests are also taken to guide the best treatment options.
At the end of this appointment your healthcare professional team will:
- Give you their contact number
- Arrange your next appointment
It is OK to call while you are waiting for results, if you want to ask questions or have concerns.
While waiting for results, if your baby is eligible, please get your baby’s Medicare number (for those in Australia). This will help you access treatment once you have a diagnosis.
Diagnostic testing & understanding SMA genetics and inheritance.
SMA is an inherited genetic condition.
What are genes = Genes are found in every cell. They are like the blueprint for our body. They contain instructions for things like what colour our eyes are, or how tall we might be.
What are proteins = If genes are the blueprints, proteins are the bricks and builders. They are crucial to the instructions being carried out.
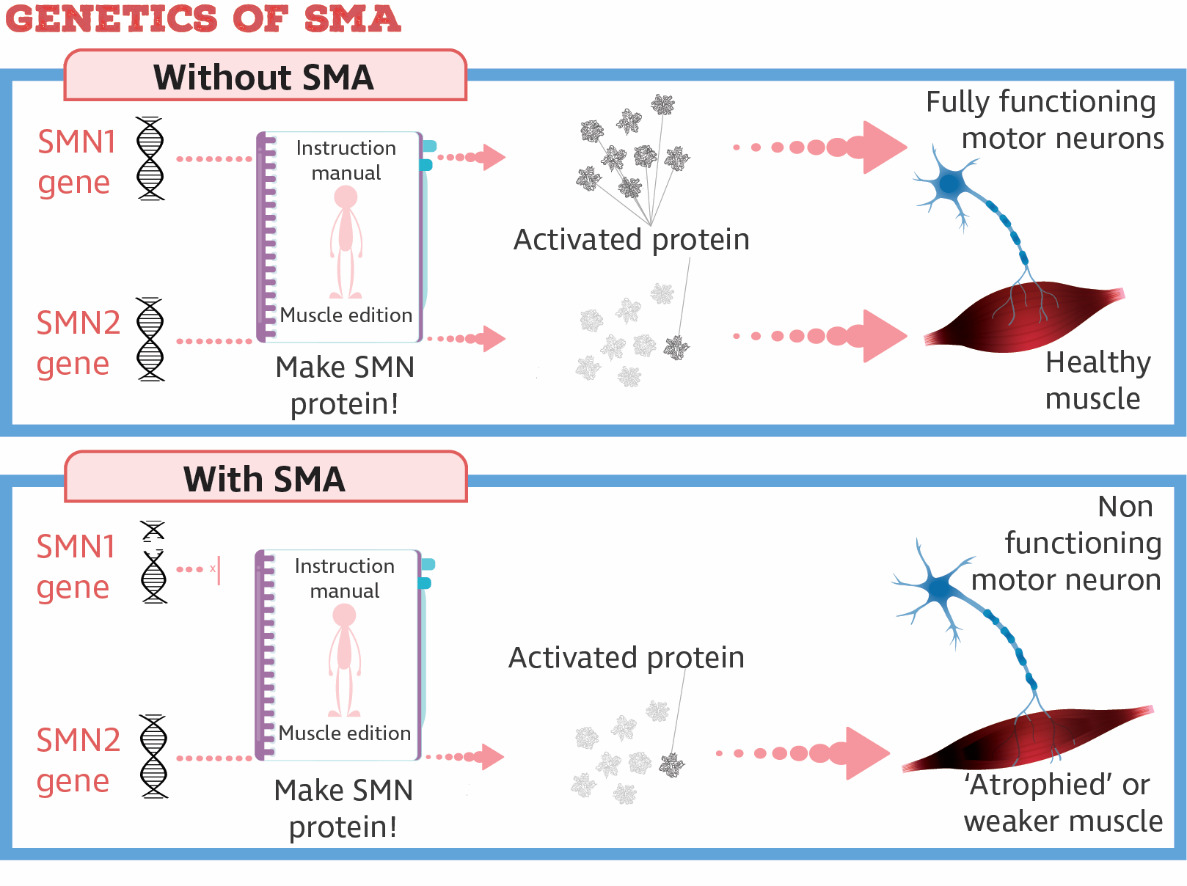
Everyone has a gene called the survival motor neuron 1 gene (SMN1). SMN1 is important because it makes a protein called survival motor neuron (SMN). If we don’t make enough of this protein, we lose motor neurons, until they can no longer send messages to muscles to move.
Most people have two working copies of the SMN1 gene. SMA occurs when both are not working. In 95% of people with SMA this is because part of the gene is missing, or deleted. This is what newborn screening helps identify. A second blood test is done to confirm the deletion in the SMN1 gene and the diagnosis of SMA.
There is another test that can tell us about how SMA can impact your baby. This test looks at SMN2, not SMN1. SMN2, or survival motor neuron 2, is like a backup to SMN1. But this backup can only make a small amount of the protein SMN1 is normally responsible for. This is not enough to stop the disease.
The number of SMN2 genes varies between individuals. Counting these tells us if the disease will be more or less severe. This helps us make choices about which treatment is best for your child. We call this SMN2 copy number. As soon as your baby’s results are known, your healthcare team will contact you and make a time for your next appointment quickly.
SMN2 helps to predict how severe the weakness might be, without newborn screening or treatment, and can help to predict the response to treatment:
- The most severe form appears from birth, and kids have only 1 copy of the SMN2 gene.
- Without treatment, kids with 2 copies of SMN2 developed symptoms in the first weeks of life, called ‘early infantile onset SMA’ (SMA type 1).
- Without treatment, kids with 3 copies of SMN2, developed symptoms in infancy or childhood (SMA types 2 or 3, or ‘later infantile onset SMA’)
- For people with 4 copies, symptoms can appear at varying ages (SMA types 3 or 4)
The health care team will talk about genes and inheritance when they have diagnostic test results for your baby. Sometimes parents ask questions about SMA and their family sooner.
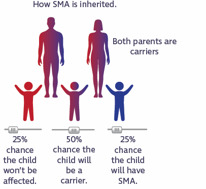
Parents of a child with SMA are often “carriers”. This means they each have one fully working SMN1 gene, and no symptoms. About 1 in 50 people are carriers of SMA, but often people don’t know it. A DNA test is the only way to find out. If both parents are carriers, there is a 1 in 4 chance that each of their kids can have SMA.
A genetic counsellor will help organise your carrier testing after your babies genetic tests are available and when you are ready.
As a reminder, you have no control over the genetic information you pass on. No one causes gene variants, and they cannot be prevented. You did not cause this to happen.
2.a. What does this mean if I have older children? Could they also have SMA?
Your health care team will speak with you about any other children you have. There is a small chance that they could be health carriers of SMA, which may have implications when planning a family of their own. There is a smaller chance that a sibling might be affected – your doctor will discuss whether any other children need review by a neurologist or genetic testing.
2.b. What are the implications (if any) for my future kids? And my kids’ kids?
A genetic counsellor will help you consider these implications and will be able to discuss the risk of having another affected child. There may be implications for your other kids and their kids. A genetic counsellor will help you work out who else in your family might need to be tested.
2.c. Who else should be tested in my family?
Once the results of your “carrier testing” are available, a genetic counsellor will meet with you to work out who else in your family might need testing. This might include siblings of yourself and your partner.
Autosomal recessive is a term used by geneticists to refer to the way in which an inherited disease is passed down within a family. When two parents are unaffected healthy carriers of a genetic condition, they have a 1 in 4 chance of having an affected child. SMA is inherited in this way.
5% of individuals with SMA have a different genetic change in the SMN1 gene. It interferes with the function of the SMN1 gene, but is not detected by the technology used in the newborn screening test.
NB: If you have questions about the specifics of your carrier status your team/genetics counsellor can provide more information